

The extensor tendons are very vulnerable in wounds on the dorsal side of the hand, as they lie immediately beneath the skin.
The anatomy is very simple in the wrist and back of the hand, but very complex in the fingers.
There are two types of extensor tendons:
- extrinsic extensors, whose muscular body is located in the forearm and ends in a long digital tendon.
- intrinsic extensors, whose muscular body is located in the hand itself and inserts directly onto the metacarpals.
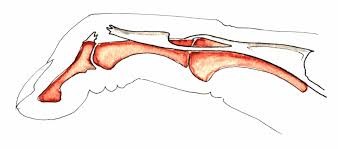
We can only really speak of a tendon on the dorsal surface of the wrist and hand, because at the digital level it’s more of a thin tendinous blade with a complex architecture.
The mechanism of finger extension is very complex:
- the extensor digitorum communis and the extensor digitorum proprius of the II and V ensure extension of the metacarpophalangeal joint M.C.P., and assist extension of the I.P.P. and I.P.D.
- the medial band extends the proximal interphalangeal joint, I.P.P., and the terminal band extends the distal interphalangeal joint, I.P.D.
- the intrinsic muscles participate in the extension of the I.P.P. and I.P.D.
- the thumb has independent tendons with the specific function of orienting it in relation to the other fingers: the long extensor of the thumb, the short extensor and the long abductor, short abductor.
CLINICAL SIGNS
The diagnosis of a lesion of the extensor apparatus can only be clinical, and requires a precise examination by a competent and vigilant partner.
The classification of the International Federation of Societies of Hand Surgery provides a reference for dialogue, as well as a therapeutic correspondence for each topography.
Testing of the extensor apparatus is fundamental; it must be analytical or even counter-resistant:
- Metacarpophalangeal extension tests the common extensor and extensor tendons of the long fingers.
- Proximal interphalangeal extension essentially tests the medial strip, while being wary of possible compensations.
- The distal interphalangeal extension study enables the lateral and terminal bands to be studied, and is performed in M.C.P and I.P.P extension.
- The extensor pollicis longus is tested with the hand flat on a table, and the patient is asked to lift the thumb towards the ceiling. The extensor pollicis brevis is tested using active extension against resistance of the M.C.P.
The presence of finger deformity in the initial phase of trauma is inconstant and depends on the extent of the injury, as well as on the flexibility of the injured person.
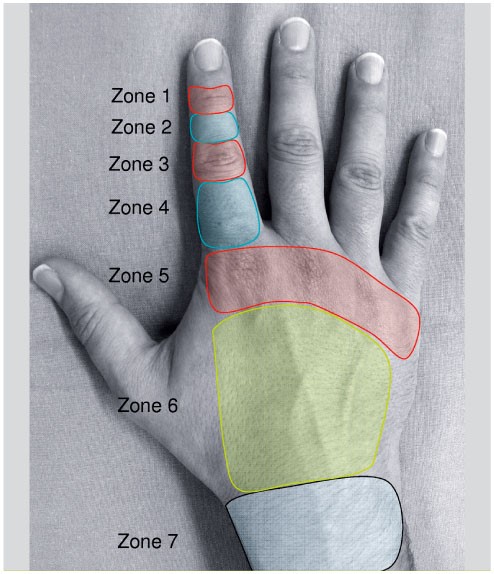
Classification for diagnostic and therapeutic purposes
Two types of deformation are characteristic:
- The “buttonhole” deformity, related to a section of the medial band at the back of the I.P.P. There is permanent flexion of the I.P.P. and permanent extension of the I.P.D., flexible and reducible at first.
- Mallet-finger” deformity, caused by sectioning of the two lateral bands or the terminal band. There is irreducible flexion of the I.P.D. Later, disruption of the extensor apparatus can lead to a “swan-neck” deformity, with hyperextension of the I.P.P. and permanent flexion of the I.P.D.

TREATMENT
Treatment requires surgical repair.
After cleaning and excision of dirty surrounding tissue, the tendon is sutured sufficiently firmly to allow rehabilitation.
When the lesion is located very close to the bone insertion, trans-osseous reinsertion is required. In the case of loss of tendon substance due to decay, it is preferable to graft rather than suture at the cost of shortening. Skin coverage is a fundamental parameter. In the case of contusion, rasping or major damage, loss of skin substance should be treated with a skin-covering flap to facilitate tendon gliding.
Immobilization in a thermoformed plastic splint generally lasts three weeks, followed by basic rehabilitation.
EVOLVING RISKS
Associated lesions, particularly skin lesions, are important prognostic factors for functional recovery.
The risk of stiffening is real, and may require tenolysis or even tenoartholysis at a later stage, to free the repaired tendon that is sticking to its vicinity.
