
Kienbock’s disease is defined as aseptic necrosis of the semilunaris (a bone belonging to the first row of the carpus) without any notion of trauma.
The factors incriminated in the genesis of this disease are :
- hyperpressure of the radius on the semi-lunate bone
- vascular fragility of the semilunaris

VASCULAR VARIANTS OF THE SEMILUNATE
Clinical features:
Clinical signs are not specific, but should raise the diagnosis, especially in young adults who present with wrist pain associated or not with some stiffness and, above all, a loss of grip strength with pain localized on the semilunar.
Additional work-up :
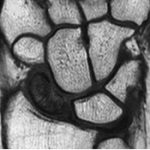
Standard X-rays of the wrist from the front and side may be normal in the early stages: if there is any doubt about the diagnosis, an MRI or CT scan should be carried out; these examinations will show a difference in contrast or bone alterations in favour of incipient necrosis in the semilunar region.
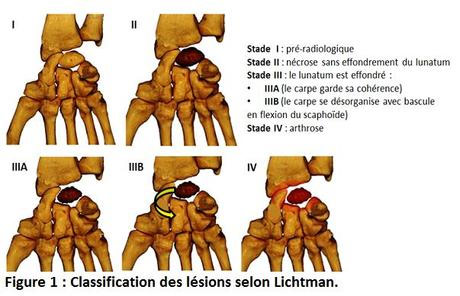
Kienböck disease is classified according to the “Lichtman” radiological stages:
Kienböck disease is treated surgically: in the absence of surgical treatment, the clinical and radiological signs will worsen, with no timeframe given for the passage through the various stages.
The decision to preserve the semilunaris depends on the radiological appearance of this ossicle and the stage of the disease.
- Techniques preserving the semilunar bone: the aim is to reduce the pressure exerted on the semilunar bone if there is a difference in length between the two bones of the forearm, a shortening osteotomy of the radius is most often performed.
- if the two forearm bones are of equivalent length, reduce the height of the greater bone: this “opens” the semilunar compartment from below,
- arthrodesis of the lateral column: by partial arthrodesis between the scaphoid and the trapezoid pair, or between the scaphoid and the greater bone: this will increase the height of the carpus below the height of the radius and consequently reduce the pressure exerted on the lunate.
- modification of the radius inclination; either verticalization or horizontalization: both techniques can significantly modify intra-carpal pressure.
- revascularization of the lunate: microsurgical techniques.
- techniques to excise the lunate: these are indicated when the architecture of the lunate is too altered
- replacement of the lunate by the pisiform or by a prosthesis
- resection of the first row of carpal bones: This is a classic procedure, which involves excising the three ossicles of the first row of carpal bones to create a joint whose second row articulates with the radius. The result is a stable, mobile and strong wrist.
The various procedures may be combined with :
- carpal denervation (wrist desensitization)
- emptying of the cancellous bone at the distal end of the radius (reduces pressure).
The choice of surgical technique depends on a number of factors, including
- age; profession,
- stage of the disease,
- whether or not the two forearm bones are unequal in length
- a pathological radial slope,
- whether there is associated wrist osteoarthritis.
The post-operative course varies according to the technique used.
Your surgeon will give you all the information you need on the choice of procedure (depending on the diagnosis and stage of the disease), its progress and after-effects, and the expected benefits.
