
Ulnar impaction syndrome (UIS) is the result of a positive ulnar variance, i.e. the ulna is too long in relation to the radius. This inferior rdio-cubital index is measured on frontal X-rays using several methods.
The long ulna may be congenital or acquired.
Over the course of a lifetime, the ulna tends to “descend” during effort, and the distal radio-ulnar index becomes more positive over time.
CLINICAL:
Pain on the medial side of the wrist (opposite to the thumb side), particularly when loading the wrist or tilting the wrist ulna. Loss of strength is common.
RADIOLOGICAL EXAMINATION:
Clinical examination is essential, supported by static and dynamic X-rays of the wrist. Plain X-rays are sometimes normal, except in the case of distal radius fracture sequelae. It is important to take profile X-rays of the forearm to check that the radius and ulna are parallel. Any subluxation of the ulna, usually posterior, should be noted.
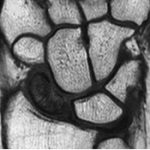
Arthroscanner+++ or MRI may be useful, and may show :
usually central, degenerative perforations of the triangular ligament, cartilage erosions of the proximal dome of the semilunate and triquetrum.
This ulnocarpal and, secondarily, distal radioulnar osteoarthritis is the cause of the pain. Normal X-rays mean that pain can be ignored for a long time.

MEDICAL TREATMENT:
- Resting the wrist and avoiding certain activities.
- Analgesics and anti-inflammatories.
- Cortisone infiltration
SURGICAL TREATMENT:
All these procedures result in decompression of the carpus, with most of the forces passing back through the radiocarpal joint, and the pain disappearing. Results in terms of prono-supination are variable.
- Ulnar shortening osteotomy: indicated when the distal radioulnar is well-oriented, congruent and non-arthritic.
- The ulnar shortening osteotomy will be directional, with an anterior-based wedge resection if the ulna is subluxated posteriorly.
- The Darrach procedure consists in removing 12 mm of the distal ulna. This resection must be accompanied by arthroplasty and stabilization of the remaining ulnar shaft. Fibrous interposition, closure of the capsule and resetting of the E.C.U. tendon should be part of the same operation.
- Or sometimes radius lengthening osteotomy, depending on the case.

