Whether traumatic or following tumor removal, the loss of skin substances is defined according to their location, area, depth, elements exposed or affected by the loss of substance.
All the elements may be involved in a loss of substance: bone; muscle; tendon; vascular pedicle and nerve.
Substance loss reconstruction is scheduled based on the exposed features and the urgency of their coverage. The loss of a noble element also affects the timing of reconstruction and the priorities of the elements to be rebuilt first.
If the direct suturing devices fail due to loss of the substance, the skin is covered by (skin graft) or by a loco-regional or remote fat or musculo-cutaneous flap.
Preparing the bed for loss of substance before repair remains the critical step for successful coverage. The choice of hedge depends on local factors and the size of the substance loss. Local resources, if available, are used first. Coverage is by “the simplest to the most complicated” means.
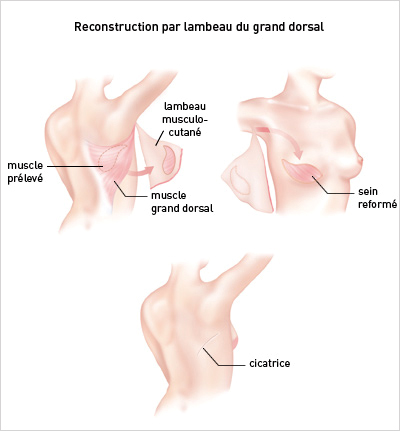
Example: Breast reconstruction after tumor removal:
Flap reconstruction uses your own tissues (skin, fat, muscle) to replenish the breast, moving them from another part of the body (back, tumy).
Different types of flaps are used depending on the case: the flap of the great dorsal muscle, the flap of the great rectus muscle of the abdomen or a flap of skin and fat taken from the abdomen called DIEP.