In an emergency, the examination of a hand or wrist wound is difficult because of the pain and the often significant bleeding. As a result, the rule of thumb is that all hand wounds located in the anatomical path of a tendon, nerve or artery must be surgically explored under good technical conditions. All injuries, and nerve injuries in particular, must be repaired.
Wounds on the wrist or hand pose different problems:
- At the wrist, it affects mixed sensory and motor nerves:
The ulnar nerve is located medial to the artery beneath the tendon of the ulnar flexor carpi muscle. It gives a sensitive branch for the dorsal hemiface of the wrist, then divides into a sensitive branch for the last fingers and a deep motor branch which controls the interosseous and hypothenar muscles, etc.
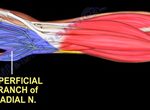
The median nerve is very superficial; it gives the palmar cutaneous branch for the base of the thumb, then at the exit of the carpal tunnel, motor branches for the thenar muscles of the thumb and sensory branches for the first four fingers.
- on the hand, the wound involves only pure sensory nerves:
the digital nerves are exclusively sensory, originating either from the ulnar or median nerve. At the distal part of the palm, these digital nerves divide to take charge of the sensitivity of a hemi-finger. These nerves run along the palmar surface of the finger, superficial to the arteries, and terminate in a distal, pulpal arborescence.

Clinical signs
At the wrist, the median nerve is superficial and therefore highly vulnerable. A section of the median nerve results in paralysis of the external thenar muscles, i.e. paralysis of the opposition of the thumb to the other fingers, and anesthesia of the pulps of the first three fingers and the outer half of the ring finger. Ulnar nerve transection results in anaesthesia of the ulnar hemi-pulps of the ring and little fingers, combined with complete paralysis of the intrinsic muscles of the fingers (e.g. inability to spread the fingers apart or bring the 5th towards the 4th). High transection also implies loss of sensitivity of the dorsal hemi-face of the wrist.
In the hand, damage to a digital nerve or, more distally, to a digital collateral nerve, results exclusively in loss of sensitivity in the territory concerned. Damage to the major hemi-pulps is functionally detrimental.
Associated lesions, particularly tendinous and arterial, must be repaired at the same time, but often pose additional technical and prognostic problems.
Complementary examinations
The diagnosis is exclusively clinical:
- the interview notes the conditions of the injury:
on the wrist: this is often the result of a serious glass wound, e.g. after putting your hand through a window or door, or a suicide attempt with a razor or knife, etc.
on the hand or finger: more often a domestic accident; pitting fruit, slicing ham, opening oysters during the festive season…
- testing of the various pulps to look for hypo or anaesthesia of a territory. It is the search for a motor defect in a digital segment that suggests a motor nerve lesion, but once again: the rule is that any hand injury located on the anatomical path of a tendon, nerve or artery must be explored surgically under good technical conditions. All injuries, and nerve injuries in particular, must be repaired.
Treatments
In the wrist, the technique for repairing the median and ulnar nerves depends on whether there is contusion or loss of substance.
Direct suturing can be performed as an emergency procedure if the wound is clean and straightforward, with no loss of substance. Peripheral sutures are performed under a microscope or high-magnification magnifier, using a very small 9/0 or 10/0 thread (100 microns) and precise microsurgical instruments. The addition of biological glue reduces the number of sutures, ensuring better coaptation of the two ends and perfect sealing of the nerve sheath.
All associated lesions are repaired at the same time. Arterial repair is essential for trophicity. Lesions of the flexor tendons are then repaired with precise post-operative procedures.
When direct suturing is impossible, with contusion of the extremities, it is important to locate these extremities and bring them together with a few stitches to avoid retraction, limit conjunctival scarring and enable secondary repair.
Secondary suturing is possible if, after resection of the extremities, the distance is short and suturing can be performed without excessive tension, with the joints in extension.
Fascicular nerve grafts can be used to bridge longer gaps, usually using the sural or short saphenous nerve.
On the hand, all lesions are repaired in the same order as wrist wounds: tendons, nerves and arteries. After regularization of the extremities without intra-nerve dissection, the fascicular groups are identified and the suture is epiperineural, taking in the connective envelopes en bloc, using 3 to 4 stitches and biological glue. (Visco)arterial repair improves nerve recovery and pulpal trophicity. Immobilization lasts 15 days, but from the 10th day onwards, nerve and artery healing allows controlled passive mobilization in the case of associated tendon lesions. Nerve grafting is possible in fresh lesions with loss of substance, if local conditions allow, as sensory nerves are paucifascicular. Good local coverage may require a local flap. In the case of an isolated nerve lesion, the grafts used are a branch of the musculocutaneous nerve, or the short saphenous nerve if there are several lesions.
The prognosis
Functional outcome depends on the type and level of injury, the existence of associated lesions and their treatment, and the age and characteristics of the patient (e.g. smoking).
Assessment is carried out in the clinic using simple, reproducible techniques, comparing the opposite side and neighbouring fingers. Progression is marked by the appearance of a Tinel’s sign (painful percussion of the distal progression of nerve regeneration), the return of voluntary motricity, sensitivity and sweating. Given the speed of nerve regeneration (1mm/day on average), the minimum recovery time is 6 months, with improvement possible up to 18 months.
Sensitivity can be divided into 4 stages, from complete anesthesia to protective sensitivity, then tactile and finally discriminative. Tact is explored through accurate recognition of the hemipulps, and discrimination with monofilaments.
The return of motricity begins with muscle tone, sensitivity and trophicity. Subsequently, voluntary muscle contractions reappear. For the median nerve, we look for antepulsion/opposition of the thumb, and for the ulnar nerve, abduction-elevation of the little finger, clawing and fingers in flaps, and spreading-grasping of the fingers.
The electromyogram detects the onset of recovery by showing subclinical reinnervation potentials.
The risks
The major risk is not to repair a nerve lesion due to ignorance or lack of exploration. In the case of a recent nerve trunk wound, primary suturing performed in a specialized center by a trained operator under good technical conditions has specific indications: sections of purely sensory or motor branches, particularly in the hand; partial lesions of mixed sensory-motor nerves, where primary suturing is relatively simple, in contrast to secondary repairs; and all clean wounds with no loss of substance.
Contused wounds and/or those with a large loss of nerve substance are treated secondarily with nerve grafts.
