

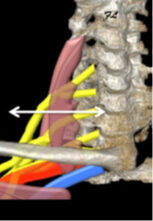
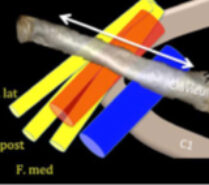
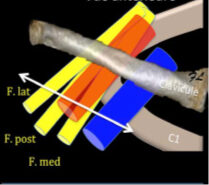
Cervicothoracic outlet syndrome corresponds anatomically to compression of the brachial plexus and subclavian vessels in a narrow passage formed by the interscalene outlet and the costo-pectoral space. There are many causes of this problem. Very often, they are functional forms linked to posture, with horizontalization of the clavicles, or to breast hypertrophy. More rarely, there are anatomical causes, such as the presence of a more or less complete supernumerary rib. The presence of a cervical rib is observed in less than 1% of the population, and is 9 times out of 10 asymptomatic.

Clinical signs:
Anatomical elements are compressed during elevation of the upper limb, typically to reach an object on a shelf or hang laundry.
Clinical forms vary widely:
- Purely vascular forms are revealed by exertional ischemia, phlebitis of an upper limb, distal embolism or even Raynaud’s syndrome. These forms account for around 5% of all cases.
- Purely nervous forms are also rare; there are high and low forms, manifesting as pain due to damage to a nerve trunk of the brachial plexus, with tingling or numbness-type paresthesias, sometimes even with motor paralysis like an “ulnar claw” due to damage to the C7-C8 roots.
- The mixed form is the most common, but also the most difficult to diagnose. It is characterized by pain in the arm and a sensation of increased heaviness when the arm is raised; patients cannot hold their arms up for long.
Diagnosis is based above all on questioning and clinical examination.
A number of manoeuvres can be used to identify vascular problems.
Adson maneuver: The test consists of rotating the head on the side being examined, chin up, arm externally rotated and slightly abducted (30°), accompanied by deep inspiration. The test is positive if the radial pulse disappears on the affected side.
Wright’s test: The limb under examination is placed in external rotation and abducted 180°. In this position, we look for radial pulse disappearance, paresthesia and pain.
Allen test: Arm externally rotated 90°, abducted 90°, chin lowered and turned contralateral. Positive test if radial pulse disappears, paresthesia or pain appears.
Eden or Falconer test: patient stands at attention, externally rotates and retropels the shoulder to close the costo-clavicular space. Positive if radial pulse disappears, paresthesia or pain appears.
Roos maneuver: The patient places himself in the “hands up” position and performs opening and closing movements with his hand. The test is positive if symptoms appear before 40 movements or less than 3 minutes. Wright’s Adson and Roos maneuvers reveal a damping or disappearance of the radial pulse and a muscle cramp.
Areas of compression are often :
Complementary examinations :
Pulsed Doppler ultrasound enables us to study the subclavian vessels and look for aneurysmal narrowing or dilatation, given that a murmur corresponds to a narrowing of more than 50% in caliber.
Two positive clinical tests and a positive Doppler scan establish the diagnosis.
Standard X-rays of the cervical spine look for the presence of a rib or supernumerary rib stump.
Electromyograms are rarely significant, except in obvious nerve forms with established sensory-motor paralysis.
MRI is not very helpful, and spiral angioscanner may be useful.
Treatment of cervicothoracic outlet syndrome:
Treatment is essentially functional, with appropriate rehabilitation.
The aim of this re-education is to open up the defilement and the costo-clavicular clamp. Results generally take time to achieve, and maintaining them requires adequate physical maintenance.
Surgical treatment is only required for obvious forms of deficiency, or when an anatomical obstacle has been identified. The cervical approach is mainly used for neurological forms involving resection of a cervical rib, fibrous tract or middle scalene. The Ross axillary approach is reserved for vascular forms requiring resection of the 1st rib.
