
Obstetric brachial plexus palsy (OBPP) is a partial or total paralysis of the arm and hand, caused at birth by damage to the nerves at the root of the arm. It is visible from birth, affecting one in every 2,000 newborns. Depending on the nature of the lesion, spontaneous recovery is total (disappearance of the paralysis), partial or nil (definitive paralysis: partial or total).
WHAT IS THE BRACHIAL PLEXUS?
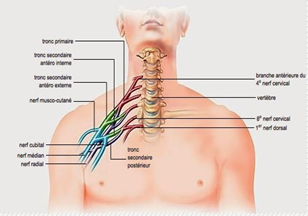
The two brachial plexuses are networks of nerves located roughly at the base of the neck, from which the nerves innervating the upper limbs originate. Each is made up of the last four cervical nerves (from the cervical spinal cord, known as roots C5 to C8) and the first dorsal root (D1). Some forms reach all the roots, others only some.
HOW DOES POPB MANIFEST ITSELF?
At first, the newborn has an inanimate arm (paralysis usually affects only one arm). There has often been a difficult delivery (large child, forceps delivery, difficult shoulder passage, obstetric maneuvers, etc.).
Once the diagnosis has been made, a medical check-up can identify the damaged nerve fibers with some precision, without however being able to establish the exact nature of the damage.
Complementary examinations are possible: X-rays can detect associated lesions (broken clavicle, etc.); electromyograms assess the electrical activity of the nerves and localize lesions (after the end of the first month); myelography (special X-ray of the spinal cord) looks for characteristic signs of nerve damage. In the case of severe damage, this examination helps to localize and assess the nature of the damage.
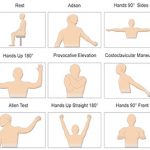
The picture is highly variable:
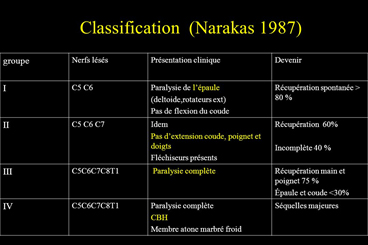
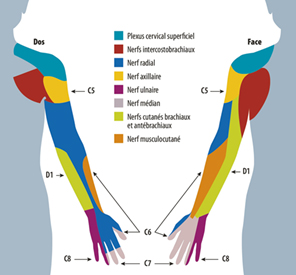
- in cases of high paralysis (75% of cases), the shoulder is inactive, the arm is inert along the body, the wrist can be touched, the hand functions correctly.
- The paralysis then affects the C5-C6 and sometimes C7 nerve roots (C5-C6 involvement is called Erb-Duchenne paralysis);
- in the case of low paralysis (reaching C8 and D1), in addition to the arm, the hand is partially or totally affected;
- total paralysis (C5 to D1) is fairly rare and definitive.
- other disorders are possible: sensory, vasomotor (pale limb), associated fracture (clavicle, humerus), diaphragm involvement (if C4 is involved – difficulty breathing), Claude-Bernard-Horner syndrome (eye involvement).
WHAT ARE THE CAUSES?
It is during difficult deliveries that nerves are damaged, as a result of excessive traction on the head when releasing the child, whether he or she is pre-sent by the head or by the breech (buttocks first) to free the head or arms. Extreme traction stretches the nerves: three types of nerve damage are observed: stretching, rupture and tearing.
HOW DOES IT EVOLVE?
In the early days, it is very difficult to make a prognosis. Spontaneous recovery (by nerve regrowth) depends on the lesions. A large number of POPBs will recover (those caused by stretching) within the first few weeks.
Massive recovery is seen before the age of 3 months. For other cases, which can lead to irreversible paralysis, it’s only after three months that a precise assessment can be made to distinguish between partial recovery, which will be the subject of continued physiotherapy treatment, and non-recovery, which will indicate surgical intervention from the 4th month onwards.
Restorative or palliative surgery may then be considered.
After six months, muscles that have not fully recovered never return to normal. Final disability depends on recovery. In the most critical cases, neither the arm nor the hand will be able to function. In the majority of cases, only the hand will be able to function normally, with the arm’s mobility and strength more or less reduced. Paralysis, if it persists, does not worsen. But complications may set in: muscle retractions, contractions, osteoarticular deformities, a “forgotten” limb. Muscular retractions and imbalance in shoulder muscles must be prevented, and joint mobility preserved.
POPB does not appear to be painful for newborns. Discomfort (pain, tingling) has nevertheless been reported by adults suffering from brachial plexus paralysis (caused by accidents).
WHAT TREATMENTS AND CARE CAN BE OFFERED?
Prevention
This involves detecting the disproportion between the size of the unborn child and the size of the future mother’s pelvis, by ultrasound or other means, prior to delivery. In cases of obvious disproportion, which can be confirmed by radiological measurement of the size of the pelvis, a Caesarean section should be performed. In borderline cases, vaginal delivery can be attempted, with a caesarean section if necessary. Predictable birth weights of over 4 kg, difficult previous births and a family history (on the mother’s side) require careful monitoring.
Treatments
The child should be monitored from the very first weeks. Useful treatments include: physiotherapy (daily sessions during the period of spontaneous recovery, mainly in the first year) and after any surgery;
temporary postures (bandaging, splints); electrical muscle stimulation; nerve grafts (not before the third month, but preferably from the 4th month onwards; the grafts are taken from the child); muscle transfers; palliative surgery (elimination of uncomfortable postures or unsightly movements, e.g. due to muscle retraction).
ROLE OF FAMILY AND FRIENDS
In the case of persistent paralysis, physiotherapy is required for several years, until the child is fully grown. To avoid becoming a parent-caregiver, professional help is recommended. Parents should :
- evaluate the relevance of the proposed interventions and involve the child in the choices,
- let the child explore his or her limits in physical activities (avoid overprotection),
- encourage autonomy, if necessary through occupational therapy,
- to answer or have answered the child’s questions about his or her trauma (meeting other carriers of this paralysis, objectives of care…).
