

Deep wounds on the palmar surface of the hand can cause injury to the flexor tendons.
The prognosis and treatment outcome of tendon injuries differ fundamentally according to the site of injury.
The reference anatomical classification divides the wrist and hand into distinct zones, each characterizing the position of the two tendons, the deep common flexor (FCP) and the superficial common flexor (FCS), and their relationship with adjacent structures.

Zone I: Downstream of the terminal insertion of the FSD (flexor digitorum superficialis), i.e. about halfway down P2, encompasses the distal insertion of the FPD « flexor digitorum profundus ».
Zone II: Begins at the distal palmar crease (where the FSD and FPD tendons cross in the sheath = decussation zone) and ends at the distal insertion of the FSD bands on the middle part of P2. This is Bunnel’s « no man’s land » zone, characterized by a narrow osteo-fibrous canal, tight flexors and precarious vascularization. Zones I and II form the digital canal.
Zone III: Palm area, starting at the exit of the carpal tunnel and ending at the distal palmar crease, i.e. at the entrance to the digital canal.
Zone IV: Zone corresponding to the carpal tunnel.
Zone V: Forearm zone. Begins at the flexor muscle-tendon junction and ends at the entrance to the carpal tunnel. Zones 3, 4 and 5 are characterized by good tendon vascularization and a much freer tendon course. This classification also applies to the thumb, where there is only one tendon, the flexor pollicis longus (LFP), with better vascularization.
Clinical signs
Questioning should clarify the nature of the vulnating agent and, above all, the position of the finger at the time of injury. On an injured finger in flexion, the distal end of the severed tendon is more distal than the skin opening, and the proximal end is much more proximal, retracted into the palm, attracted by the force of contraction and the elasticity of the muscle body. A functional study of the hand and fingers reveals the lesions:
- The first phalanx (P1) is flexed by the interosseous muscles, the second phalanx (P2) by the FCS and the third phalanx (P3) by the FCP.
- The first phalanx must be maintained in extension to eliminate overall finger flexion managed by the interosseous muscles.
- The FCP is explored by blocking P2 in extension to eliminate the action of the FCS.
- Exploration of the FCS is performed by immobilizing the healthy fingers in extension, which prevents the action of the FCP of the injured finger. Associated lesions must be taken into account as they affect the prognosis:
- The existence of a contusion or precarious skin flap runs the risk of necrosis or local disunion. Loss of skin substance requires coverage with a locoregional flap.
- Osteoarticular lesions are evidence of significant trauma, leading to adhesions and stiffness. Treatment must enable early mobilization.
- Nerve damage is common at all levels. A stiff, unresponsive finger is highly detrimental to overall hand function.
- Vascular lesions must be systematically repaired, as good local vascularization is a major guarantee of a good trophic result.
Treatment
The approach uses the wound itself, after trimming the edges, enlarged at the ends in a zig-zag pattern using the Bruner technique.
- Zone 1 long fingers :
Isolated sections of the FPD should be repaired by direct suture; there is no impact on SDF function. Active flexion of P3 is better than tenodesis or arthrodesis.
If the section is very close to the distal insertion, transosseous reinsertion provides solid fixation and enables very early rehabilitation.
- Zone 2 long fingers:
Note the importance of proximal tip retraction, as “whiplash” rappels pull out the vinculae.
There are two main types:
– Favorable cases, with a clear cutaneous lesion, frank tendon section without retraction of both ends and intact vinculae, integrity of the floor of the digital canal, or even an isolated lesion of a nerve or collateral bundle. Both flexors must be sutured and the pulleys respected.
– The suture must be strong to ensure good tensile strength
– The suture must preserve tendon glide by ensuring that the two ends meet perfectly and that the suture thread is as fine as possible.
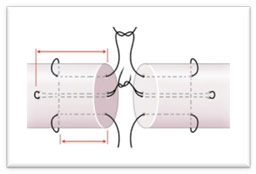
– Surgery must respect the epitendon and vinculae, which are the feeder vessels. When the proximal end of the tendon does not appear at the level of the digital canal wound, blind manoeuvres must be avoided to prevent tearing the mesotendons. The tendon can be pushed back into its sheath by massaging the muscular body and flexing the wrist and fingers. Sometimes, a proximal counter-incision is necessary to recover the retracted end; the tendon will be drawn to the suture zone by a flexible silicone tractor. Suturing procedures are varied, with either a Kessler or Kleinert frame, or longitudinal, or with a Tsuge-type support loop.
To regularize the suture zone, either a peri-tendinous suture using 7/0 very fine thread, or a circular fibrino-bonding procedure, is required.
The sutures are protected by a dorsal anti-brachio-palmar splint. This immobilization, with the forearm pronated, wrist at 30°, MP at 40° flexion and IP in slight flexion, is maintained for at least 3 weeks in permanent wear, and 2 to 3 weeks at night.
Rehabilitation is undertaken immediately post-operatively, except in the case of vascular-nervous lesions, where a one-week delay is applied.
Duran’s method consists in manually and passively mobilizing the joints distal to the tendon section in the splint from D0 to D21, followed by a phase of active aided and then active global mobilization of the fingers from the immobilization position, without ever bringing the finger to maximum extension, thus avoiding any excessive traction on the tendons.
Increasingly, the current trend is towards controlled early active mobilization to promote mobility, while accepting the risk of breakage.
Thumb:
Wounds on the palmar surface of the thumb are characterized by the frequency of associated vascular and nerve lesions.
Immobilization is provided by a dorsal ante-brachio-palmar splint, with the thumb in antepulsion, wrist and metacarpophalangeal flexion.
Rehabilitation follows the same Duran technique.
Specific risks
Lesions of the flexors are serious injuries, with a major risk of retaining a mobility deficit, either in flexion or extension.
Associated bone, neurovascular or skin lesions have their own consequences, but have a negative impact on the final result.
In the majority of cases of isolated flexor injury
Re-education should be carried out at an early stage, with the patient’s informed participation, respect for precautionary instructions and patience.
