

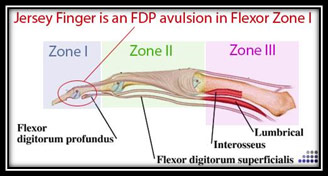
This is a distal rupture of the terminal tendon of the flexor digitorum communis profundus (F.C.P.).
Its etiology is mainly sports-related, particularly contact sports such as rugby. It most often affects the fourth finger.
It is often operated on too late, as it is too often initially unrecognized. It’s the classic phenomenon of grabbing the shirt of an opposing player during a tackle in rugby.
During a forcé flexion grip, there is a sudden hyperextension of the tip of one finger, particularly the fourth, while the others are flexed.
The muscular body is in a phase of maximum contraction and the torn tendon will retract, sometimes far upstream of its physiological insertion.
What are the clinical signs?
In recent avulsions :
The patient presents with painful impotence of the I.P.D. The pain was sudden, tracing all along the flexor, going up to the palm or even the forearm.
Palpation of the digital canal is painful, sometimes with ecchymosis on the finger.
Active flexion is impossible.
Palpation of a painful swelling, localizing the retracted flexor tendon tip, is an inconsistent sign.
In old avulsions :
Active bending of the I.P.D. is impossible.
Grip is very limited.
I.P.P. flessum may occur if the torn tendon is trapped in the decussation.
Palpation may reveal swelling extending into the distal palmar crease.
A classification taking into account the degree of tendon retraction and the possible existence of a bone fragment:
| Type I : the most frequent type in recent lesions |
The distal tip is located in the decussation of the F.C.S. in front of P1 The long vinculum is intact A small avulsed bone fragment from P3 may be blocked in the decussation |
| Type II : it tends to deal with old traumas |
The distal tip is upstream of the decussation in front of the MCP or even in the palm. Devascularization is complete, with all feeder vessels torn off. |
| Type III : a rare form |
The rupture is accompanied by a large fragment of P3, a true articular fracture with dorsal subluxation of P3. Retraction is virtually nil, due to the size of the fragment. |
A standard front and side X-ray of the finger and hand is the basic examination, to look for any bone fragments. Its size and location are assessed.
In the case of older lesions, an ultrasound scan can be very useful in assessing the extent of tendon retraction.
Treatment:
In the case of recent injuries < 21 days, tendon reinsertion of the F.C.P. on P3 should be attempted first and foremost.
In old lesions > 21 days, the therapeutic indications will depend not only on the level of retraction and joint flexibility, but also on the extent of functional discomfort, loss of muscle strength, and patient motivation.
If the retraction is very significant and fixed, particularly in the case of palm retractions, the choice is between tendon grafting or an operation to fix the I.P.D. by tenodesis or arthrodesis, depending on the patient’s discomfort and motivation. The aim is to provide a stable, solid joint in a functional position (10-15°).
