

Paresthetic cheiralgia, or compression of the sensitive branch of the radial nerve at the wrist, associates pain on the radial edge of the hand, sensitivity disorders in the sensory territory of the radial, and a “pseudo-Tinel” at the point of emergence of the nerve.
Pain is aggravated by hyperextension, pronation and ulnar deviation of the wrist. How can this branch be compressed?
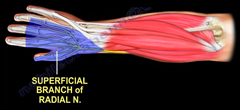
The sensitive branch of the radial nerve (BSR) detaches from the radial nerve trunk at the elbow, runs along the deep surface of the long supinator muscle (BR) and emerges from the antebrachial aponeurosis between the first radial (ECRL) and the long supinator (BR). In depth, it rests directly on the radius. Its point of emergence is approximately at the junction of the lower third and upper two-thirds of the forearm. The tendons of the first radial and the long supinator form an “open pair of scissors” distally, between the blades of which the radial emerges. The “pair of scissors” is open during supination and wrist extension, when the nerve is relaxed. It closes on the nerve and can compress it in pronation and wrist flexion, as well as in ulnar deviation.

Several etiologies are possible:
- All repetitive movements of wrist extension – flexion – ulnar deviation (striking with a hammer) and pronation – supination (using a screwdriver).
- Compression of the BSR directly on the hard bony plane of the radius by an external object: jewelry bracelets or watch straps (which can also compress the dorsal cutaneous branch of the ulnar nerve).
- Handcuffs can also play this role (prisoner’s paralysis).
- The compressive syndrome of the BSR may also reflect mononeuritis, and diabetes should be investigated.
- De Quervain’s tenosynovitis may itself lead to damage to the BSR.
- A local anatomical variant of the long supinator (BR): several authors have described an anatomical variant (present in 3% of a series of 150 Turkof dissections) in which the BSR emerges from the fascia through a duplication of the long supinator.
- Other, rarer causes have been described: ganglions, cysts, lipoma, fracture sequelae, locoregional injection sequelae, AIDS, spider bites, etc…
Symptomatology
Pain is almost always the reason for consultation. It is located on the radial edge of the hand, and its location is not always clearly defined by the patient. It is aggravated by wrist movements and gripping (both grasping and key pinching). It is rarely nocturnal, unlike the usual ductal syndromes. Painful dysesthesias or paresthesias are not always present. The perception of normal subjective sensitivity (whereas specific tests often show disturbances) is due to the fact that in 3 out of 4 patients, the terminal branches of the musculocutaneous nerve contribute to innervation of the dorsum of the first commissure. The appearance of the hand is normal. There is no vasomotor disorder suggestive of algodystrophy or Sudeck syndrome.
Palpation reveals a painful point at the junction of the distal and proximal thirds of the forearm.
Percussion of this point, located proximal to the first extensor slide, causes paresthesia and tingling on the dorsum of the first commissure: this is the irritative or pseudo-Tinel syndrome.
Sensitivity testing: effleurement, tuning fork, pricking/touching, discrimination of the two static points, microfilament test (Sammes-Weinstein) shows alterations compared with the opposite side.
As with De Quervain’s stenosing tenosynovitis, the Finkelstein test is positive: flexion of the thumb in the palm, flexion over the thumb of the long fingers and ulnar deviation of the wrist cause pain on the sensitive branch of the radial nerve and paresthesia in the corresponding territory.
The Dellon and Mackinnon test is more specific: hyperpronation of the forearm with the wrist in neutral position. The test is positive if painful paresthesias in the cutaneous territory of the radial appear after one minute.
Diagnostics
- De Quervain’s stenosing tenosynovitis:
The symptoms associated with this condition are very similar to those of paresthetic cheiralgia, so clinically it’s easy to confuse them. Moreover, these two conditions can occur simultaneously, and even more so: stenosing tenosynovitis can cause irritation of the sensitive branch of the radial, and surgical release of the abductor longus and extensor pollicis brevis tendons can suppress neurological symptoms.
The intertwining of these two pathologies should not, however, blind us to the specific signs of each:
- In de Quervain’s tenosynovitis, there is an inflammatory phenomenon: crackling sounds are felt when the tendons concerned are actively mobilized. There may be edema, redness and warmth, and the symptomatology is classically located in line with the radial styloid, opposite the first groove, where there is an arch. Finkelstein’s sign is positive. Ultrasound or MRI scans show enlarged tendons, sometimes with fissures, and sheath effusion.
- Paresthetic cheiralgia is at least initially a compressive phenomenon, and the pain point is more proximal than in stenosing tenosynovitis. Above all, there is a genuine local irritant sign: percussion of the SSB causes paresthesia in the corresponding skin territory.
Blocking the BSR at its point of emergence can be a useful procedure to differentiate between frankly doubtful cases, but it is only reliable if the block is high and performed precisely in contact with the nerve.
- Compression of the sensitive cutaneous branch of the musculocutaneous nerve at the elbow:
For the reasons outlined above (overlapping innervation territories), symptoms can be very similar. A block of the MC at the elbow, in the external bicipital groove, will clarify the etiology of the disorders.
Further tests
The electromyogram may show a slowdown in the speed of sensitive conduction between the elbow and wrist, and a reduction in the amplitude of SSB action potentials. A positive EMG reinforces the diagnostic hypothesis, but a normal examination does not rule out the reality of local compression. Diagnosis is above all clinical, however, and the sensory blocks described above are generally more than sufficient to pinpoint the level of injury.
Treatments
- Treatment is initially conservative, since there is no risk of motor impairment developing. Infiltration of a cortisone derivative can be used to hasten healing, which always takes a long time. Per-osmo and local anti-inflammatory treatment can be combined with a wrist and thumb orthosis, and skin desensitization sessions. TENS current can be effective, and is always worth a try because of its innocuousness.
- Surgical treatment is intended for late-onset cases, cases where conservative treatment has failed and traumatic cases:
- If the injury is linked to an identified local compressive process, this must obviously be removed. – The aim of the operation is to free the BSR. The skin incision will be staggered in relation to the path of the nerve to avoid skin scarring over the neurolysis area.
- Any untimely manipulation of the nerve should be avoided, and only an epineurotomy performed a priori. The susceptibility of this nerve a priori contraindicates extensive interfascicular neurolysis.
- If necessary, partial resection – particularly if there is a local anatomical variant with a supernumerary or duplicated tendon – or total resection of the brachioradialis tendon can be performed.
- In the case of iterative revision, some authors have described the possibility of a graft, but the final solution is sectioning of the BSR upstream of its point of emergence. The proximal stump must be buried in the deep surface of the brachioradialis muscle body.
Conclusion:
The identification of Wartenberg syndrome prior to surgical treatment of de Quervain tenosynovitis is essential. It can prevent unpredictable post-operative complications. By taking into account the history of the disease through accurate questioning and careful clinical examination, the value and outcome of the chosen treatment are highly predictable.
