
Anterior interosseous nerve syndrome: this is the rarest form of compressive neuropathy affecting the median nerve. It is a purely motor neuropathy characterized by loss of thumb-index terminal pinch.
Involvement of the anterior interosseous nerve is easily confirmed by EMG.
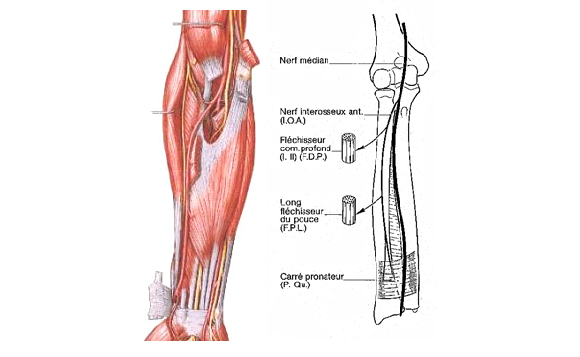
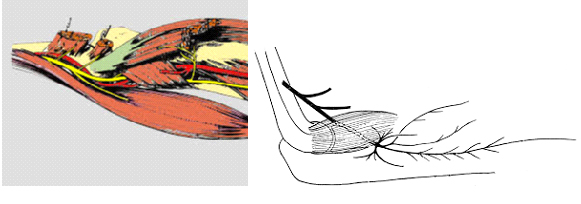
The median nerve gives rise 5 to 8 cm beyond the epi trochlea to the anterior interosseous nerve, which innervates the flexor pollicis longus, the radial part of the flexor digitorum profundus and the pronator quadratus. This nerve has no sensory territory.
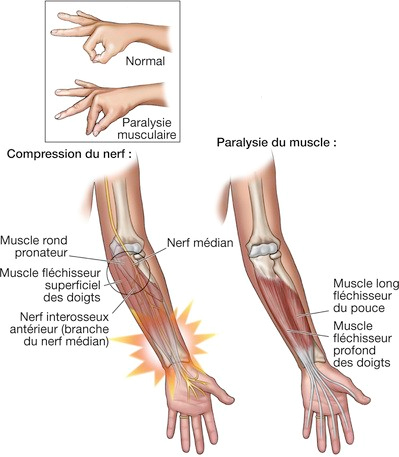
Three potential sites of compression for the median and anterior interosseous nerves at the elbow and upper forearm: the fascial expansion of the biceps towards the epicondyle (lacertus fibrosus); the crossing of the pronator teres (pronator teres); and the insertion arch of the flexor digitorum superficialis.
Clinical signs:
Diagnosis is often delayed, as the deficit may go unnoticed for some time. It is usually preceded by a period of pain in the forearm, sometimes radiating to the wrist, lasting from a few days to a few weeks, which may be aggravated by movements, particularly prono-supination.
A complete deficit results in lack of flexion of the interphalangeal joint of the thumb, combined with lack of flexion of the distal interphalangeal joint of the index finger. Damage to the pronator quadratus branch is impossible to diagnose precisely, due to the simultaneous compensatory action of the pronator teres.
The characteristic sign of complete damage is the impossibility of making a circle with the terminal pollicidigital forceps, which then become laterolateral, giving a “duckbill” appearance.
In some cases, flexion of the distal interphalangeal joint of the medius may be affected at the same time.
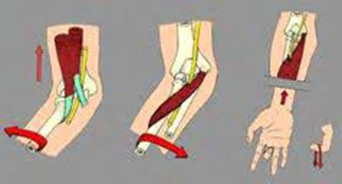
Clinical examination may reveal pain on deep palpation of the forearm, especially in the early stages. The three Spinner tests can be used to sensitize this examination:
– Supination against resistance, elbow bent, awakens pain by tensioning the lacertus fibrosus on the nerve.
– Pronation against resistance compresses the median between the two heads of the pronator teres.
– Flexion of the proximal interphalangeal joint of the medius, by contracting the flexor digitorum superficialis, leads to compression by the arch of this muscle.
Complementary examinations :
An MRI scan may be performed. While it may reveal an etiology or a non-specific inflammatory or scarring zone, it can never confirm the diagnosis with certainty.
The electromyogram alone will be decisive. This is difficult in this pathology, as the finger flexors must be studied separately.
Treatment:
Treatment may initially be medical. In fact, it should be reserved for forms with known medical causes (viral, inflammatory), which are rare, and its duration should be limited in time: 6 to 8 weeks. It involves wearing a resting splint and prohibiting certain gestures that load the nerve on a muscular arch.
Surgical treatment may be proposed immediately if the electrical study is positive.
This involves dissecting the median nerve in the forearm from the flexion crease of the elbow to the middle third of the forearm, and releasing the areas of compression.
The posterior interosseous nerve:
Commonly referred to as the motor branch of the radial nerve, the posterior interosseous nerve is actually a mixed nerve. Its motor contingent enables wrist and finger extension, and participates in thumb abduction and supination movements. The sensory contingent concerns the distal portion of this nerve, terminating at the dorsal aspect of the wrist.
The posterior terminal branch of the radial nerve gives rise, almost immediately after its origin, to a branch to the short extensor carpi radialis muscle, belonging to the outer lodge of the forearm.The posterior interosseous nerve carries downwards, outwards and backwards, entering the supinator muscle two centimetres below the elbow joint. Its entry into the supinator muscle is marked by a fibrous arch described by Frohse. It thus wraps around the radial head.

It then reaches the posterior region of the forearm, running between the superficial and deep chiefs of the supinator, which it innervates. The PIN emerges from the supinator near the lower edge of the muscle, through the interstice separating its two layers. It thus arrives between the two muscular planes, superficial and deep, of the posterior antebrachial lodge. At this level, the NIP immediately gives rise to:- posterior branches for three of the superficial muscles of the posterior lodge: the extensor digitorum communis, the extensor digitorum proprius and the extensor carpi ulnaris;- anterior branches for the four muscles of the deep plane, from medial to lateral: the extensor digitorum proprius, the extensor pollicis longus, the extensor pollicis brevis and the abductor pollicis longus.
From the lower third of the forearm, it runs along the posterior surface of the interosseous membrane, whose fibers are directed downward and inward, with the exception of the more distal fibers, which are directed upward and inward. The posterior interosseous nerve, on the posterior surface of the wrist, engages under the dorsal annular ligament of the carpus, and opens out into numerous articular threads that terminate in the radiocarpal, carpal and carpo-metacarpal joints.
Clinical signs:
Posterior interosseous nerve syndrome often results from compression of the radial nerve, when its motor branch penetrates the supinator muscle beneath Frohse’s arcade, a fibrous arcade on the surface of the muscle fibers. By thickening of this arch, it should be noted that compression can be tumoral (lipoma, etc.) or traumatic (wound, Monteggia dislocation, etc.) in origin.

Symptoms include deep pain in the posterior aspect of the forearm, tingling, numbness in the posterior aspect of the wrist and hand, and rarely radial paralysis, manifested by a deficit in finger extension associated with radially inclined wrist extension.
Surgical treatment consists of sectioning the superficial portion of the supinator muscle and the fibrous arch (Frohse’s arch) that compress the nerve.
Anaesthesia: usually local anaesthesia (arm anaesthesia)
Scars: closed with a few absorbable threads buried under the skin (invisible). Located on the outside of the elbow, 4 to 5 cm in length.
Post-operative follow-up: outpatient hospitalization (a few hours). Dressings for 10 days, showers as soon as dressing is removed, on day 10. Showers possible with waterproof protection.
Pain rare and mild, well soothed by usual analgesic treatment.
3 weeks off work. No sport for one month.
