

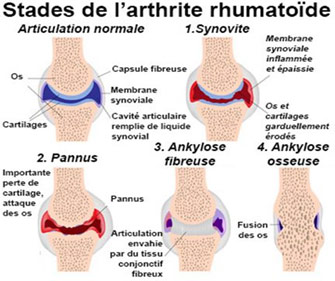
Rheumatoid arthritis is a specific inflammatory rheumatic disease that primarily affects synovial tissue, with joint destruction and deformity appearing as the disease progresses.
The disease can affect all joints, with hand and wrist involvement present in 75% of patients, characterized by highly disabling deformities at a distance from the primary involvement.
All forms of synovial involvement can be seen, but the most frequent are :
- articular synovial involvement with capsular and ligament distension
- peritendinous synovial involvement of wrist and finger flexors.
- The dorsal synovium may be affected, with progressive destruction of the tendons.
Due to the particular anatomy of the hand, proximal deformity of the wrist leads to downstream deformity of the fingers.
Rheumatoid wrist:
Deformities affect :
- The radioulnar joint, with posterior dislocation of the ulnar head and forward dislocation of the posterior ulnar tendon.
- The carpal joints, with intracarpal misalignment and reduced carpal height.
- Ultimately, joint damage results in fusion of the carpal bones (“fusing carpus”).
- The radiocarpal joint, with the carpus sliding along the articular slope of the lower end of the ulna. This deformity is accompanied by a radial inclination of the wrist and a compensatory “ulnar gust” of the fingers.
Finger deformities:
In rheumatoid arthritis, the initial cause of pain and deformity is the inflammatory development of the synovium (synovitis). Very often, this synovitis disappears thanks to general medical treatment (background therapy, anti-inflammatories) or local treatment (infiltrations). On the contrary, if it resists medical treatment, it can lead to tendon rupture, ligament distension or joint destruction.
Flexor tendons:
Inflammatory thickening of the tendon sheaths hinders tendon movement, resulting in a protruding finger. Swelling is often visible and even palpable on the palmar surface of the fingers and wrist.
Synovitis distends the pulleys of the digital canal and may infiltrate the tendon. When synovitis is severe, it can lead to tendon rupture, making it impossible to flex the finger.
Finger joints:
Intra-articular synovitis leads to ligament distension and cartilage damage. The joint becomes unstable, then subluxated, leading to imbalance in the finger chain.
In the metacarpophalangeal (M.C.P.) joints, deformities are characterized by ulnar deviation due to dislocation of the extensor tendons in the intermetacarpal valleys, and palmar subluxation due to modification of the flexor axis.
at the level of the proximal and distal interphalangeal joints (I.P.P and I.P.D), we observe 3 types of deformity which may be associated:
- Swan neck: hyperextension of the I.P.P. and flexion of the I.P.D.
- Buttonhole: accompanied by hyperextension of the M.C.P., flexion of the I.P.P. and sometimes hyperextension of the I.P.D. The deformity is initially supple, but may stiffen.
- Mallet finger: this corresponds to flexion of the I.P.D. and may accompany swan-neck deformity.
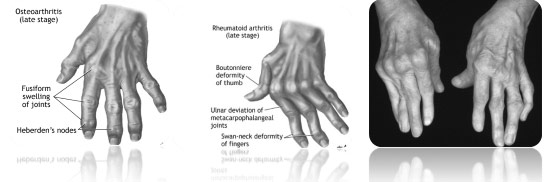
In the thumb, the deformity is either flexion of the metacarpophalangeal joint and extension of the interphalangeal joint, giving a “Z” thumb, or extension of the M.C.P. and hyperextension of the thumb’s I.P., with very awkward closure of the first commissure.
Complementary examinations:
Standard comparative radiographs are required
For the wrist, one face and a strict profile.
For the hand, one face and a three-quarter view to assess palmar dislocation of the M.C.P.
Treatment of deformities in rheumatoid arthritis:
The application of therapeutic means must be organized in the form of a treatment plan. the implementation of a basic medical treatment and its monitoring.
A number of corticosteroid infiltrations may be considered, depending on the number of joints affected. If this fails, synoviorthesis is the preferred option.
If a deformity becomes established or progressively appears, early surgical intervention should be considered to avoid destruction of capsulo-ligamentary structures, tendons and joints.
Synovectomy:
Indicated when synovitis is resistant to medical treatment. The operation is performed outside the main inflammatory periods, under regional or general anaesthetic, usually on an outpatient basis. There is no splinting after the operation, and rehabilitation begins immediately. Removal of the synovitis protects progression and also has a pain-relieving effect.
- Synovectomy of the extensors is the most common procedure. Synovitis may infiltrate the inferior radioulnar joint. It is therefore often combined with an articular procedure as part of a Sauvé-Kapandji-type operation with ligament stabilization.
- Metacarpophalangeal synovectomy is proposed to avoid deterioration of the extensor tendons and deformities. It is an on-demand procedure, sometimes combined with capsulo-ligamentary stabilization.
- Synovectomy of I.P.P. joints is rarer, and must be performed very early if a gain in mobility is desired.
- Synovectomy of the flexors is often required when there is compression of the median nerve in the carpal tunnel. Synovectomy can be performed on each finger to avoid tendon rupture.
Synovectomy of thumb joints must be performed early to avoid deformity and instability.
Ligament and tendon interventions:
Proposed to restore the correct position of the wrist and hand. They are most often associated with synovectomy or joint surgery.
at wrist level, the anatomical situation of the posterior ulnar tendon, dislocated at the front, needs to be re-established. Tying off part of the dorsal annular ligament is the basic procedure, combined with an articular procedure after synovectomy, either a Sauvé-Kapandji-type procedure (osteotomy of the ulnar head and restoration of continuity by fixation of the ulnar head to the distal end of the radius), or a Darrach procedure (resection of the ulnar head). If the carpus begins to dislocate at the ulna, transferring the tendon from the 1st to the 2nd radial will reduce the risk of aggravating this deformity.
In M.C.P. joints, it is essential to re-establish a good extensor tendon strap by fixing it to the radial edge of the joint and reinforcing the joint capsule. In the presence of ulnar deviation of the fingers, the contracture of the interosseous muscles must be corrected by sectioning the tendons (tenotomy).
Swan-neck deformities are difficult to treat, and must be treated before joint stiffening, either by local plasty or plication, or by active “Littler” tenodesis.
The buttonhole deformity may benefit from surgery, after softening through rehabilitation and the use of orthoses.
Mallet fingers are treated orthopedically in the early stages; in the late stages, arthrodesis in slight flexion ensures good comfort.
Tendon ruptures mainly affect extensors, and in particular the extensor of the 4th and 5th fingers. Repair by direct suture is generally impossible, and requires grafting or tendon transfer.
Joint interventions:
Joint destruction is the terminal evolution of RA, leading to major functional impotence. It must be avoided by early intervention on the synovial pannus responsible for this destruction.
In wrist surgery, the ulnar head is either resected or fixed by arthrodesis to the adjacent radius, in order to eliminate pain, restore prono-supination and protect the extensor tendons from rupture. Total wrist prosthesis are rarely used.
Wrist arthrodesis in cases of extreme deformity, with definitive fixation of the wrist in an anatomical position using pins or a plate, possibly combined with bone grafting.
For the M.C.P, I.P.P and I.P.D finger joints, the choice is again between prosthesis or arthrodesis, depending on the degree of dislocation and destruction. A prosthesis alone is not enough to restore function; it requires an effective capsulo-ligamentary and tendinous system and good skin coverage. The preferred indication is simultaneous replacement of the last 4 M.C.P. joints, combined with repair of the extensor apparatus. I.P.P. and I.P.D. replacement is less common.
The indication is rarer in the thumb, where arthrodesis is the preferred option.
Functional rehabilitation:
Treatment of the rheumatoid hand cannot be envisaged without perfect collaboration with the physiotherapist, orthotist and occupational therapist. The methodology of rheumatoid hand rehabilitation must be gentle, cautious, painless and progressive.
Orthoses are used at every stage of the rheumatoid disease affecting the hand. The patient alternates between wearing a resting orthosis and a working orthosis. Posture splints provide comfort and limit joint deformation.
In the post-operative period, edema must be controlled to avoid sticking of the sliding surfaces, through early, active and passive mobilization of the joints, so as not to stress the newly-repaired capsulo-ligamentary structures.
Depending on the stage and structures affected by the deformity, your surgeon will suggest a treatment plan to avoid painful, deforming and destructive evolution as far as possible.

