

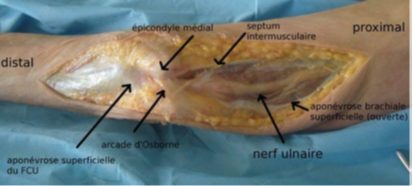
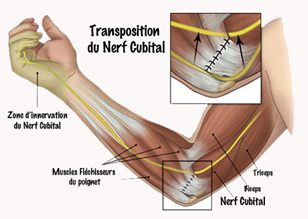
The mechanism of compression of the ulnar nerve at the elbow is very different from that of the median nerve at the wrist: this nerve passes behind the axis of rotation of the elbow in the epitrochleo-olecranial groove, then engages under various fibrous arches at the upper part of the forearm on its medial side.
The ulnar nerve is stretched when the elbow is flexed: normally, it should slide easily to adapt its length during flexion-extension movements.
Any mechanism that prevents the nerve from sliding normally will lead to signs of nerve suffering, reflected in clinical signs (which we’ll look at later): as a rule, the nerve is blocked by a fibrous arch and can no longer slide; during flexion and extension movements, it is therefore subjected to stretching that alters its cellular structure. The causes of ulnar nerve compression at the elbow vary: in more than half the cases, it occurs in the more or less distant aftermath of trauma to the elbow region (fracture, haematoma, postural compression….). In many cases, this compression is said to be idiopathic (without any specific reason).
Clinical signs
Manifestations experienced by the patient :
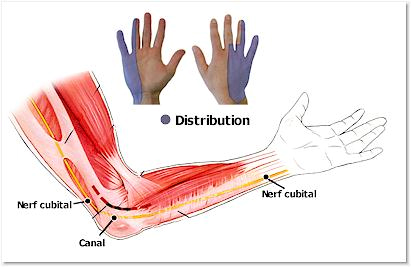
- the onset is often insidious (sometimes abrupt and precise), characterized by paresthesias (abnormal sensations) and numbness in the fourth and fifth fingers.
- Pain is very rare, and patients experience more discomfort than pain.
- Loss of grip strength is a highly suggestive sign of ulnar nerve compression at the elbow, and may be the patient’s only complaint.
- Clinical examination: looks for sensory and/or motor signs of ulnar nerve damage:
- Sensory signs: altered and/or diminished sensory perception to touch or stimulation of the pulps of the fifth and inner fourth fingers, reduced sensitivity of the dorsal part of the inner hand (compared with the opposite side).
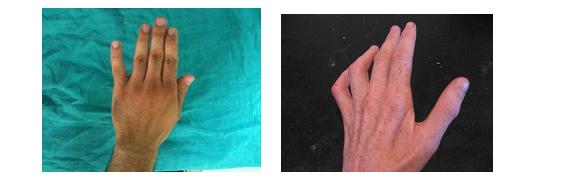
- Motor signs: loss of strength in thumb-index pinch, finger spacing and overall grip of the hand. In some cases, there is amyotrophy (loss of muscle volume) of the interosseous muscles of the hand, mainly of the muscle mass located between the thumb and index finger on the dorsal side of the hand (“1st dorsal interosseous”). -Interosseous insufficiency
- Froment’s sign
- Reducible claw deformity of the last 2 fingers
- Wartenberg sign
- Inability to cross index above middle finger
The ulnar nerve should be palpated in the groove and checked for dislocation in flexion.
Motor disorders of the fingers and thumb.
- Decreased muscle strength in the thumb-index pinch and in hand-clenching and finger-spreading.
- Amyotrophy of small hand muscles, corresponding to a reduction in muscle volume.
The onset is often insidious and slow, beginning with nocturnal tingling in the ring and little fingers. The patient often thinks he’s sleeping in the wrong position to explain the symptoms. The tingling then persists during the day, leading to a loss of sensitivity in the last 2 fingers (hypoesthesia). After several months, the motor disorders described above appear. Finally, amyotrophy appears.
Further tests
Standard X-rays of the elbow to check for fracture or osteoarthritis.
The electromyogram is the key examination: it must be carried out rigorously: its principle is to measure the speed of conduction by the nerve of an electrical stimulation: the nerve is compared to a freeway; the speed of conduction of the influx depends on the freedom of the freeway: in the event of an accident or traffic jam, the nerve impulse is slowed down: this examination confirms the diagnosis (decrease in impulse speed when passing through the elbow) and quantifies the extent of the compression (study of the trophicity of the muscles innervated by the nerve).
Treatment
As a rule, it is surgical; compressions that do not regress spontaneously must be operated on. Several decompression techniques are available: the compression zone must be lifted, and the nerve must be able to slide easily.
You can practice either :
- Simple neurolysis: simply cut the fibrous arches that prevent the nerve from moving,
- Neurolysis combined with epitrochleectomy: when simple neurolysis does not relax the nerve sufficiently, the epitrochlea must be cut to allow the nerve to roll forward, thus promoting relaxation.
Specific risks
Surgical removal of persistent ulnar nerve compression at the elbow should result in complete disappearance of clinical signs. However, this is not always the case (which differentiates this pathology from carpal tunnel syndrome): after surgical release, more or less severe tingling of the two inner fingers and/or loss of strength may persist. This is the consequence of long-standing compression, but can also be observed in the aftermath of apparently recent compression: hence the value of the electromyogram, which makes it possible to determine before the operation whether the clinical symptomatology is linked to the evolution of a chronic infra-clinical compression which may have recently decompensated (analogy with a rope rubbing against a ridge, which breaks after all its fibres have broken).
