

The osteoarticular complex of the wrist includes :
- The radial glenoid,
- The entire carpus is composed of eight bones that can be grouped into two rows, proximal and distal.
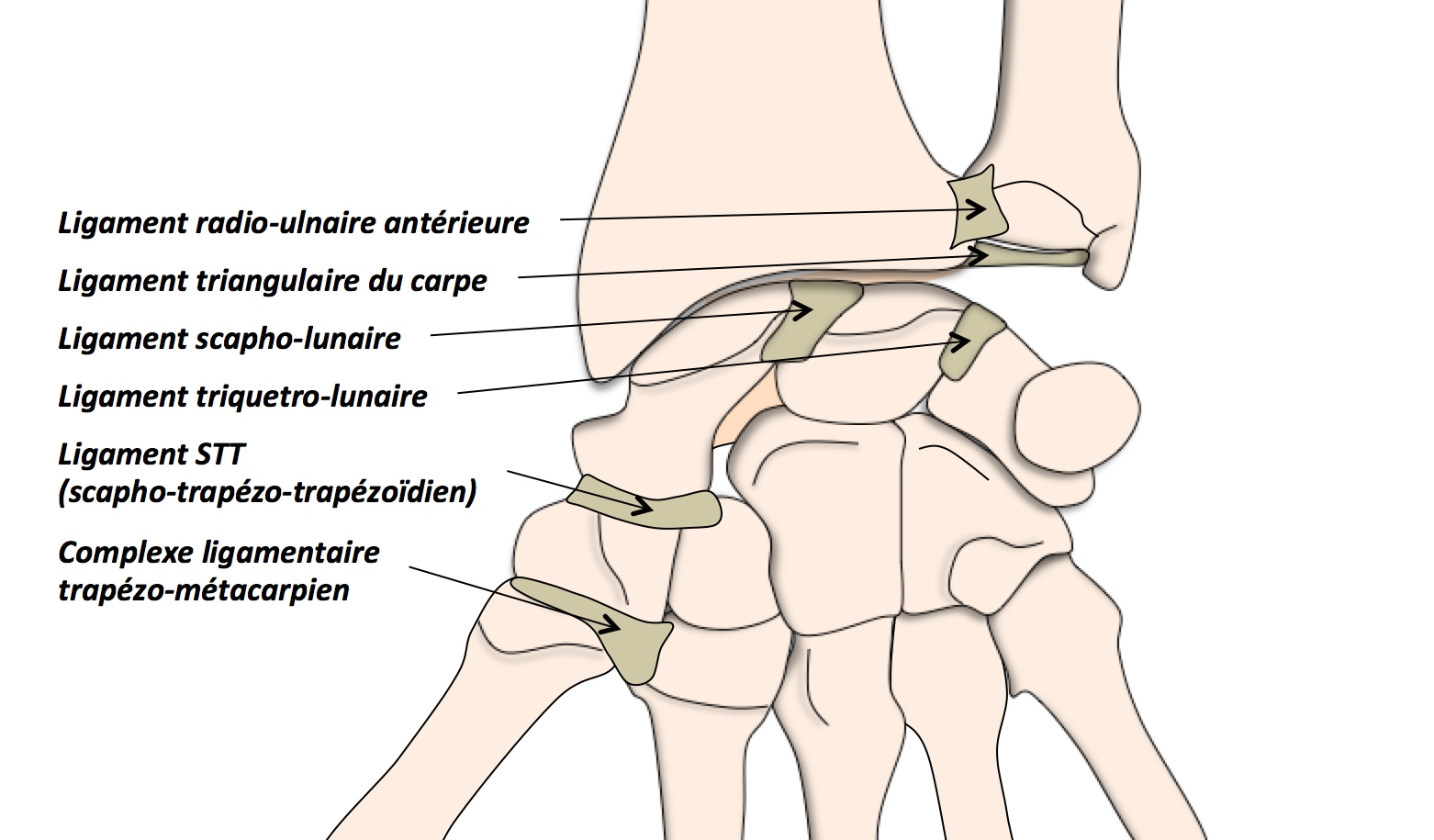
- The 33 ligaments of the wrist joint complex can be grouped as follows:
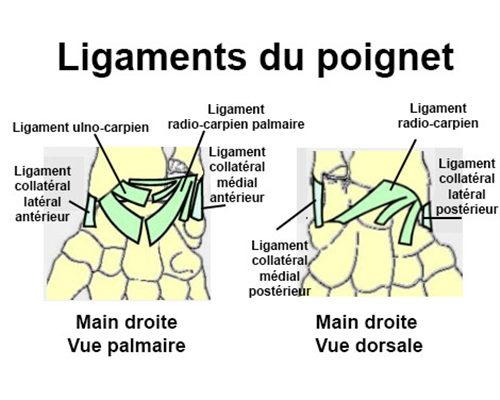
- Intracapsular ligaments, which can be divided into two groups:
- Powerful palmar intracapsular ligaments.
- Dorsal intra-capsular ligaments, relatively thin.
- Interosseous ligaments linking bones in the same row: the scapholunate and pyramidolunate interosseous ligaments are powerful ligaments, imposing close solidarity between these three bones, whose movements are always in the same direction, even if not always of the same amplitude.
The mobility of the carpal bones is coherent and coordinated:
- In dorsal flexion, the semilunar and greater bone tilt backwards and the scaphoid verticalizes. The opposite movements occur in palmar flexion.
- When tilted radially, the scaphoid becomes horizontal; when tilted ulnarly, it becomes vertical.
the three bones of the first row of carpal bones move together forwards or backwards. However, an additional shearing movement occurs at the scapholunate joint. - Loss of scapholunate coupling is manifested by a palmar tilt of the scaphoid, which becomes horizontalized, associated with a dorsiflexion tilt of the semilunar joint, which we’ll discuss later. Ligamentous lesions may be isolated, but very often they are associated with osteoarticular lesions, and the impaction component with cartilage damage worsens the prognosis (impaction of the radial styloid, isolated depressed fracture of the lunate surface of the radius, dye-punch fracture).
CLINICAL SIGNS
The clinical history is that of a young adult who has suffered a violent fall during exercise, with the wrist in hyper-extension. After a painful period of variable duration, depending on the immobilization required, the wrist resumes its function… for a variable length of time.
It is therefore often a trauma overlooked by the patient or his or her medical interlocutor, and subsequent questioning will bring up the notion of a “sprain”.
The diagnosis is then difficult when faced with a chronically painful wrist for which strength training and sporting activities have become progressively impossible.
The pain is posterolateral, found on examination at the level of the scapholunate joint line, sometimes with edema and localized synovial swelling.
Two manoeuvres are useful:
- the ballottement test.
- Watson’s maneuver, which involves applying counter-pressure to the scaphoid at its tubercle, and bringing the wrist from ulnar to radial inclination.
In physiological movement, the scaphoid lies down regularly and progressively.
In the case of a scapholunate lesion, the semi-lunate gradually lies down, but the scaphoid remains upright due to the counter-pressure exerted by the examiner.
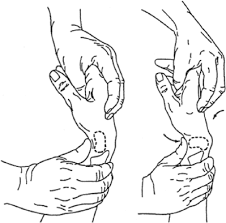
Beyond a certain radially inclined position, the scaphoid, under pressure from the trapezius and trapezoid, can no longer remain upright, and abruptly lies down.
This sudden flexion is accompanied by an abrupt, painful protrusion.
This pathological instability, unmasked by the Watson test, is responsible for the jerking and pain evoked by patients.
Gradually, patients will complain of wrist pain accompanied by a sensation of protrusion during prolonged use.
There may also be some limitation of mobility when the free interval has been long enough. After a period of several years, the complaint is essentially based on painful stiffness.
ADDITIONAL TESTS:
Initially, this lesion is not manifested by any radiographic abnormality, either on standard or dynamic X-rays, where the position of the carpal bones is not disturbed.
Complementary examinations are based on invasive imaging:
- arthrography may show a leak in the scapholunate ligament.
- the arthro-scanner is more effective, as it measures the extent of the tear, assesses the persistence of ligament stumps and looks for any associated osteochondral fracture.
- I.R.M. is disappointing so far.
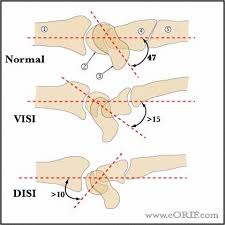
- Subsequently, the scaphoid loses its ability to straighten in ulnar tilt and wrist extension. The semi-lunate takes on its physiological resting position, i.e. dorsal inclination, where the posterior horn is thinnest.
There is thus an anterior tilt of the scaphoid and an inverse dorsal tilt of the semilunar. This appearance can be permanent on strict profile views, producing a D.I.S.I. deformity.
At this stage, complete dissociation between the scaphoid and the lunate is manifested by a scapholunate distasis greater than 3mm (Terry-Thomas sign).
The scaphoid remains recumbent and shows its distal pole: this is the Ring-sign.
This functionally troublesome scapholunate instability evolves over time into radioscaphoid and then intercarpal osteoarthritis = Watson’s S.L.A.C. Wrist.
The radiolunate joint line remains intact for a long time, but the head of the large bone may be damaged.
In the absence of treatment, pan-carpal osteoarthritis is the ultimate stage of injury, where the diagnosis is obvious on simple front and side X-rays. There is no need to ask for complicated examinations; only the assessment of the remaining healthy joint spaces is of interest, in order to propose an appropriate treatment.
In the initial stage of injury, when the diagnosis is made urgently, it is possible to offer effective, conservative treatment.
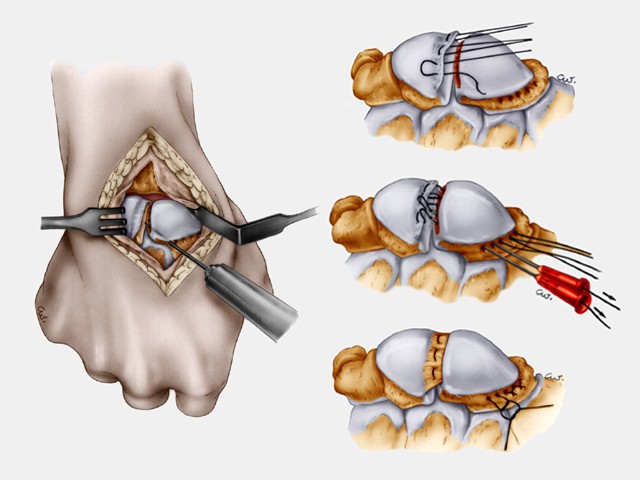
The ligament is torn from the scaphoid side, sometimes carrying a cartilaginous fragment or leaving an attached stump.
The ligament can be reinserted with transosseous stitches or stapled with anchors.
The suture must be protected with a pin and cast for 2 months.
In the later stages of chronic wrist pain, indications depend on the severity of the symptoms and the patient’s condition.
Conservative treatment may be proposed in cases of discreet dynamic instability.
Arthroscopy may also be proposed, to assess ligament damage and the condition of the joint surfaces, in addition to washing and debridement. In other cases, where symptomatic patients are in demand, or in the presence of major instability, surgical indication is unavoidable:
- Anatomical repair if instability can be reduced and the ligament stump is still suturable.
- Ligamentoplasties are delicate to perform and relax over time;
- Transposition of a free bone-ligament fragment using the techniques of A-P Weiss or Cueno, technically difficult but probably the most useful. In end-stage osteoarthritis, the therapeutic indication depends on the cartilaginous articular surfaces still intact:
- As the radioulnar joint is still intact if the head of the large bone is satisfactory, resection of the first row of carpal bones results in a pain-free wrist, retaining its pre-operative mobility and fairly well-preserved strength.
- In the event of injury to the head of the large bone, the only option is arthrodesis of the 4 internal bones, with removal of the scaphoid.
- In the case of advanced osteoarthritis involving all wrist joints, only pan-carpal arthrodesis will restore pain-free movement.
EVOLVING RISKS
The natural history of extensive scapholunate ligament rupture is now well known. After a difficult initial period, things stabilize and then progressively deteriorate, evolving over time towards radioscaphoid and then intercarpal osteoarthritis = Watson’s S.L.A.C Wrist.
The need for early diagnosis is therefore obvious; it’s what guarantees the best outcome.
Interventions are often somewhat stiffening in flexion-extension.
The risk of re-rupture after anatomical repair of the ligament is not negligible, especially if the repair was carried out at a distance from the trauma, with a poor-quality stump.
